Health Sciences
About the Research
Background

One in five children in the UK start school overweight or with obesity. This is more common in children living in deprived areas. ‘HENRY’ is an intervention to help families be more healthy to prevent children from becoming overweight. Around 24,500 families have attended HENRY since 2008. HENRY is delivered in children’s centres across the UK. In centres where HENRY is delivered, staff are trained on the HENRY approach and encouraged to provide a healthy environment. Some staff are then trained to deliver HENRY. Research that has already been done suggests that obesity levels are lower in areas that deliver HENRY. This has not yet been proved because it is difficult to find out exactly what makes obesity rates go up and down. Obesity can be influenced by things such as; the environment, our culture and the way our bodies are made. Other interventions besides HENRY might also help us to be healthy, so it can be hard to understand exactly what role HENRY might play.
Aim
The aim of this study is to find out whether children whose parents attend HENRY are less likely to become overweight or develop obesity than those that do not. We also want to find out whether HENRY gives value for money, improves the health of parents and carers that attend, benefits the staff that work in children’s centres, and has benefits to the wider community. We have already carried out some research to test whether these questions can be answered by our study (e.g., if our methods will work), and our results showed that they can.
Methods
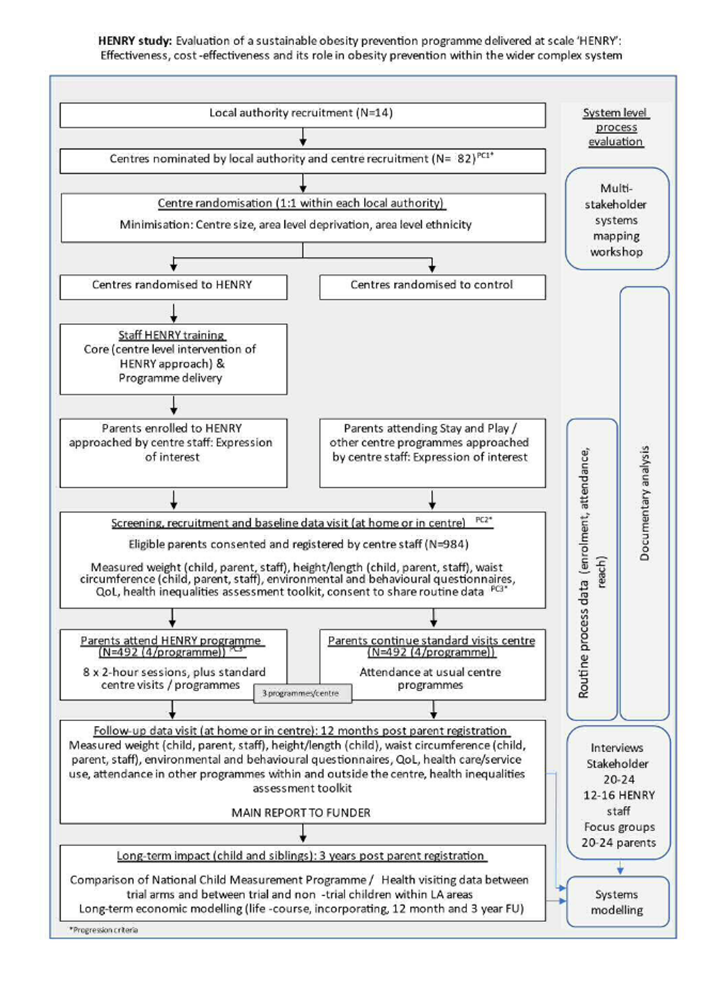
We will carry out a randomised controlled trial. Children’s centres that do not deliver HENRY will be randomly selected to either; be trained to deliver HENRY alongside standard sessions (like ‘stay and play’), or continue to offer standard sessions only. We will recruit 14 local authorities and ask each to choose around 6 of their centres to take part (82 centres total). We will then collect information from 984 families, and children centre staff from both types of centre. The data we will collect include: height, weight, waist circumference, food intake, physical activity and quality of life. We will then collect the same information 12 months later to see if there are any differences between participants from centres delivering HENRY and those that did not.

Long-term impact of HENRY
To find out whether HENRY has any long term influence on childhood obesity, we will collect data that is already routinely collected from children by health visitors and schools after 3 years. We will then compare obesity rates in those who took part in the trial to the rest of the local population.
Wider impact of HENRY
We will explore the wider influence of HENRY on obesity within local government areas and across the country. To do this, we will speak to around 60 people (including parents, health visitors, local council representatives), hold a workshop, and review documents (e.g. council strategies, planning rules).
Public involvement in the research
A group of parents with young children have already helped design our study (e.g., when and how to recruit parents). We will continue to meet with this group 2-3 times a year. One of the parents has also joined our co-applicant team.
Impact of the research
Our results will be shared with a wide range of people, including local authorities, parents, health visitors. Different delivery approaches will be planned for each group in partnership with our parent advisory group.
Study summary